Abstract
The shortage of foreign currency in Lebanon caused by the multiple crises the country has been facing since October 2019 poses a threat to the importation and availability of pharmaceutical products among other essential commodities. This has been remedied by an importation subsidy system for pharmaceuticals financed by the central bank’s foreign reserves; however, patients have recently experienced shortages of many drugs on pharmacy shelves. In this paper, we describe the pharmaceutical supply chain in Lebanon along with the subsidy system put in place by the central bank. We then propose recommendations to improve this subsidy system and enhance prescribing practices to ensure the continuous presence of medications on pharmacy shelves, and that the foreign currency supplied by the central bank is spent to the benefit of the Lebanese patients.
Introduction
Lebanon has been passing through multiple catastrophic crises since October 2019. The devaluation of the Lebanese pound, along with the unofficial capital control and shortage of foreign currency, continues to pose a threat to the importation and affordability of essential commodities. To ensure the availability of these commodities at affordable prices, the central bank has used its foreign currency reserves to subsidize a few essential commodities, including pharmaceutical products. Despite this, several pharmacies began to report shortages of many drugs starting in June 2020. These shortages might be caused by the smuggling of subsidized products outside the country, the stockpiling of chronically used medicines by patients and warehouses, and a possible delay in processing requests by the central bank. To make matters worse, a recent announcement by the governor of the central bank that the bank will be unable to continue subsidizing the importation of pharmaceuticals led to widespread panic, a rush to acquire medication refills, and possibly excessive stockpiling of medications by patients. While there is a need for an urgent plan to keep medication available at an affordable price, this plan has to be realistic and feasible. In this short paper, we describe the supply chain of imported medications in Lebanon in order to propose immediate solutions to the current crisis.
The pharmaceutical supply chain
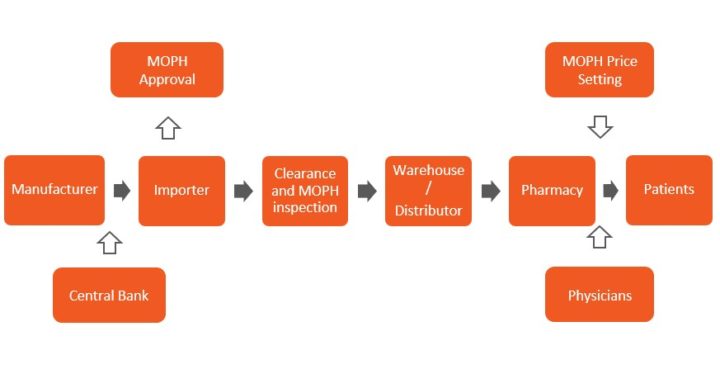
Figure 1: Diagram of the pharmaceutical supply chain of imported medications in Lebanon (Abbreviations: MOPH: Ministry of Public Health)
Only 7% of the pharmaceutical market (totalling USD 1.98 billion in 2019) in Lebanon consists of products manufactured locally. There is thus a high dependence on imported medications for the needs of residents in the country, composed of Lebanese citizens (4.9 million), Syrian refugees (1.5 million), and Palestinian refugees (192 thousand). Figure 1 describes the supply chain of imported medications from the manufacturers in exporting countries to the patient. The central bank subsidy system consists of providing 85% of the foreign currency needed for drug importation at the official exchange rate of LBP 1,500 per USD, with the remaining 15% to be bought by the importer in the black market at the unofficial exchange rate (which currently fluctuates around LBP 7,000-8,000 per USD). This has kept the supply chain going with a stable price based on the already existing pricing structure set by the Ministry of Public Health (MOPH). However, the ratio of the total amount spent on medications to GDP in Lebanon, which was quite high before October 2019, has continued to increase as GDP contracted, while pharmaceutical consumption has remained at roughly the same level. Medication spending is a large part of household expenditure in Lebanon which can be explained by the cost and high utilization of medications.
Importers then supply the distributors who store the medications in warehouses and dispense them to pharmacies based on their needs/requests. Not infrequently, the importers are themselves the distributors. Recently, the minister of public health has pointed out that drug hoarding by distributors and pharmacies, with the view of smuggling these medications outside of Lebanon or practice favouritism when selling to patients, has occurred and contributed to the medication shortage. The minister and department of pharmacist inspection at the ministry are performing raids on warehouses and pharmacies to address that. They caught and penalized certain pharmacies. However, short of addressing the root factor contributing to this behaviour, which is that the price of medications in Lebanon remains very low compared to neighbouring countries, we shall continue to witness attempts to smuggle medications. By law, pharmacists are not allowed to dispense medications that are not on the “Over-the-Counter Medications List” (OTC List ) set by MOPH without a unified prescription filled by a physician. However, in practice, pharmacists do indeed dispense many medications not on the OTC List without a prescription, with the exception of psychotropic medications. Patients then pay for these medications out-of-pocket. Those who benefit from employment funds receive partially reimbursement through the National Social Security Fund (NSSF) or some third-party payers. Those who rely on MOPH (the final safety net for Lebanese who are uninsured) can receive free medicines for chronic medical problems based on a WHO essential list of medicines, procured by MOPH and distributed to its contracted primary health care centres via the Young Men’s Christian Association (YMCA).
Any solution which aims to maintain access to affordable drugs in a sustainable manner should ensure their availability to the whole population including those with no coverage especially with the growing number of unemployed people. Such an approach can complement the drugs provided to the most vulnerable by the MOPH through YMCA.
Proposed solutions
We propose a set of reforms to ensure the continuous presence of medications on pharmacy shelves and to lessen the strain on the foreign currency reserves of the central bank. These reforms focus on reducing the cost of the subsidy system and ensuring that subsidized medications are fairly distributed to the patients who need them. The proposed solutions target two interfaces in the diagram of Figure 1: Introducing a tender subsidy and addressing the prescription system that regulates drug dispensing by pharmacies.
Amending the subsidy system:
When faced with a limited supply of foreign currency – which is the case of Lebanon today – it becomes essential to subsidize only what is needed. A review of the Lebanese National Drugs Database reveals the availability of drugs for the same ailments from different manufacturers with variable prices. All drugs imported are subsidized by the central bank at the same rate. A first step is to reduce cost by choosing to subsidize the import of the cheapest drugs without compromising on therapeutic effect. For example, there are more than 20 different trade names for the same molecule of atorvastatin – a statin medication used to prevent cardiovascular disease – and all are subsidized, even though their prices range from LBP 8,977 to LBP 42,470 for 30 tablets of 10mg atorvastatin. Subsidizing two formulations for atorvastatin chosen for their quality and lower cost can decrease the burden on the central bank, ensure all patients who are prescribed atorvastatin can acquire it, and force other importers from other manufacturers to lower their prices to be competitive in the new market. We propose two formulations per medication because, in the aftermath of the COVID-19 experience when all international supply chains were strained, relying on one supply source is not wise. Furthermore, while one formulation must be international, it is highly advisable that the other selections be from a local source. Many medications for various disease conditions are produced locally and are already available in the market. This would permit a strategic, favourable alteration of the market at many levels, supporting the local pharmaceutical industry.
The selection of the brands of medications that would be eligible for subsidies should be performed under the most transparent measures possible. ) The NSSF already has a list of medications that it covers in place. This list can be used to specify the medications that will benefit from subsidized importation. Ideally, the MOPH should conduct a study showing potential savings from adopting this strategy and use it to ensure buy-in from stakeholders such as health coverage agencies that would benefit from the resulting decrease in bills.
A more daring step to be considered later would be to perform a cost-effectiveness analysis that could then be used to choose among medicines that are not equivalent in terms of dose or therapeutic effect but are nevertheless used to treat the same clinical condition (e.g. antidiabetics, antihypertensive, and lipid-lowering agents). This will ensure the continuity of essential services. It is also important to revisit the options available all together in light of the publication of new evidence-based guidelines and market changes, such as patent expiration, in search of more affordable ones. Whether this is to be accomplished solely by the MOPH or as part of a public-private partnership programme is to be studied. One way to increase the success rate of such an endeavour would be to have an international accredited partner to work on certain areas for guidance. An example of one such area is cost-effectiveness analysis. Recent studies have identified methods to ameliorate limitations of the international applicability of established cost-effectiveness studies so they can be used in countries such as Lebanon.
As the subsidized choices become available in the market, non-subsidized options will be repriced based on the real market exchange rate. Such an arrangement will enable pharmacies to recapitalize while allowing patients who are capable and willing to pay for non-subsidized brands to retain that choice. It will also permit an assessment of the ratio of consumption of non-subsidized to subsidized brands and the planning of further reforms of the supply chain, possibly leading to tapering the subsidy system altogether for all medications within a reasonable time frame. This timeframe will be determined by several factors including the overall monetary regulations reforms and political landscape after the parliamentary elections.
| Current Subsidy System |
Proposed Subsidy System |
| All medications subsidized |
2 brand names per molecule subsidized |
| Majority of subsidized are imported medications |
1 local brand name and 1 imported brand name subsidized |
| Expensive and cheap brands subsidized |
Cheapest good quality brands subsidized |
Table 1: Comparison between the current subsidy system and our proposed subsidy system.
Enforcing prescription laws:
One of the reasons for medication shortages on pharmacy shelves is alleged stockpiling by patients and pharmacy customers at home. A pharmacy customer can purchase a majority of medications in Lebanon with no prescription. Even with the limitation on the number of doses per patient that a pharmacy can sell, patients can shop at different outlets until they acquire the desired reserve quantities. There are laws in place in place to mandate the dispensing of medications according to the quantities prescribed by a physician using a unified prescription form. Implementing these laws would be a good step towards preventing the stockpiling of medications at home. However, in the context of the coronavirus pandemic and the inability of many patients to afford regular physician visits to renew their prescriptions, asking patients to frequent their physician’s office is not always practical. Alternatives would be for MOPH to issue a ministerial decision authorizing doctor prescriptions by phone to pharmacies requested by patients. Pharmacists would document these orders in their current existing documentation systems. This would be a bold move by the MOPH towards adopting an electronic prescription system and electronic health records in coordination with the orders of physicians, pharmacists, and hospitals’ syndicate.
Digital prescribing by physicians has numerous advantages and disadvantages, depicted in Table 2 below. However, in addition to limiting patient stockpiling, digital prescribing can make tracing sales easier, thus preventing fraud, smuggling, and corruption and permitting a better analysis of consumer, prescriber, and pharmacist behaviour. This behaviour analysis would permit an evidence-based gauging of needs and enable future analyses and implementation of pharmaceutical health policies that would further improve patients’ outcomes while reducing the costs incurred by payers.
| Advantages |
Disadvantages |
| Better monitoring of pharmacy sales |
Costs of software and maintenance |
| Prevents stockpiling by patients |
Risk of inaccuracies in choosing dispensers |
| Facilitates consumer, prescriber, and dispenser behaviour analysis |
System lags |
| Provides access to patient prescription history |
Software design causing errors in filling and dispensing prescriptions |
| Overcomes problems with legibility of handwritten prescriptions. |
Requires training for prescribers and dispensers |
| Can complement telemedicine |
Security risks (Patient Privacy) |
Table 2: Digital Prescribing advantages and disadvantages (Source: US Pharmacist)
Barriers to Implementation:
Implementing the above proposals has many challenges. Subsidizing only select medications can lead many importers, those whose trade names will not be subsidized, to leave the market. This, in turn, would lead to the loss of jobs and businesses. Naturally, the pharmaceutical importer community will not welcome this. However, it may be enough to surpass this barrier if the later is coupled with two measures: a) repricing other, non-subsidized trade names based on real exchange rate market value and b) possibly permitting the export of the surplus of non-subsidized medications from the Lebanese market within 2 months of proper implementation. These measures will allow recapitalization by importers and pharmacies. Furthermore, choosing what to subsidize without a needs-based analysis will be a challenge.
The shift to digital prescriptions and use of electronic health records will require ministerial decrees for the implementation of the laws related to adopting unique identifiers for patients and electronic signatures. Lately, a turf battle has been occurring between the syndicate of pharmacies and the Lebanese Order of Physicians (LOP) over prescribing and delivering vaccines (pharmacies were permitted to administer vaccines, whereas this used solely to be the responsibility of the physician). A similar conflict could be circumvented via maintaining the financial incentive that the LOP gains from the current paper-based unified prescription. This financial incentive is income to the retirement fund, as each paper prescription has an embedded stamp worth 250LBP from the LOP. Furthermore, the MOPH, in collaboration with multiple healthcare bodies, has already proposed a road map for digital health progress, and any implementation of digital prescribing should ideally be part of that road map. Implementing this measure is furthermore facilitated by the expertise that MOPH has gained from the setup of the network of dispensaries in collaboration with the YMCA which uses electronic health records to track patients and their medication use. Expanding this existing service can be an effective quick solution.
Conclusion
Addressing the medication shortage crisis is of utmost importance as it directly affects the livelihoods of many. It is naïve to assume that the existing supply chain processes can remain effective in a subsidized system. It is similarly unrealistic to assume that the monetary condition of the country will go back to what it was before October 2019. The role of the MOPH as a regulator of each of the elements of the supply chain described above is essential. However, the above-suggested changes will also require the cooperation of the Ministry of Economy and Trade, the Ministry of Finance, the central bank of Lebanon, the syndicate of medication importers, the syndicate of pharmaceutical industries, the syndicate of pharmacies, the LOP, the consumer protection representatives, and the Lebanese parliament. All these actors are stakeholders needed for regulatory changes, smooth transitioning, and training of end-users, as well as the putting in place of an evaluation and monitoring system. Revisiting the subsidy system and enhancing prescribing practices by introducing digital prescriptions can assist in wise spending of the central bank's foreign currency reserves, ensure that what is spent is benefitting the highest number of eligible patients, and permit data generation for further optimization of processes and outcomes. However, for these changes to succeed, we cannot underestimate the need to obtain the consent of various stakeholders by minimizing the inevitable financial losses they may incur. One of the key steps to follow would be an in-depth assessment of how to ensure rational prescription practices and decrease overall pharmaceutical utilization. This needs to happen in the context of an overall reform plan for healthcare inspired by countries that have successfully managed their health sector through economic crises, such as many European countries that seized the opportunity to introduce positive changes.
The views represented in this paper are those of the author(s) and do not necessarily reflect the views of the Arab Reform Initiative, its staff, or its board.
