The Lebanese government has the responsibility to protect the health of all its citizens and residents. The early and decisive interventions implemented in the spring to address the COVID-19 pandemic allowed Lebanon to avoid what would have been an exponential rise in cases. These included thorough contact tracing, border closure, partial lockdown and (initially) centralized case isolation in hospitals.
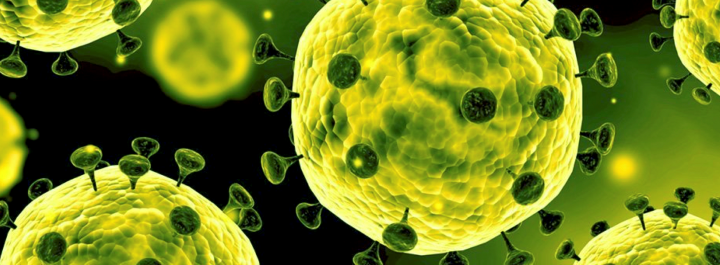
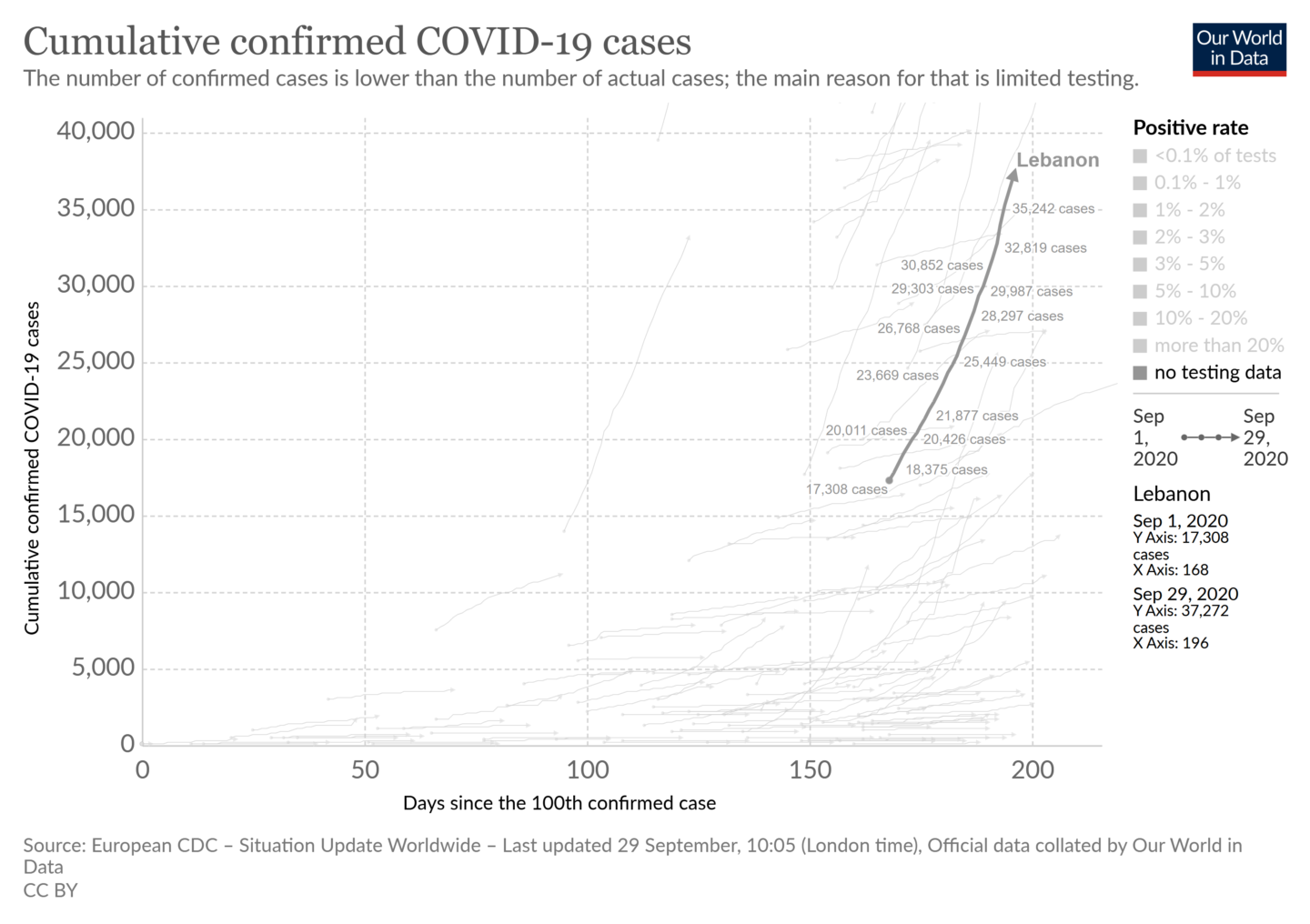
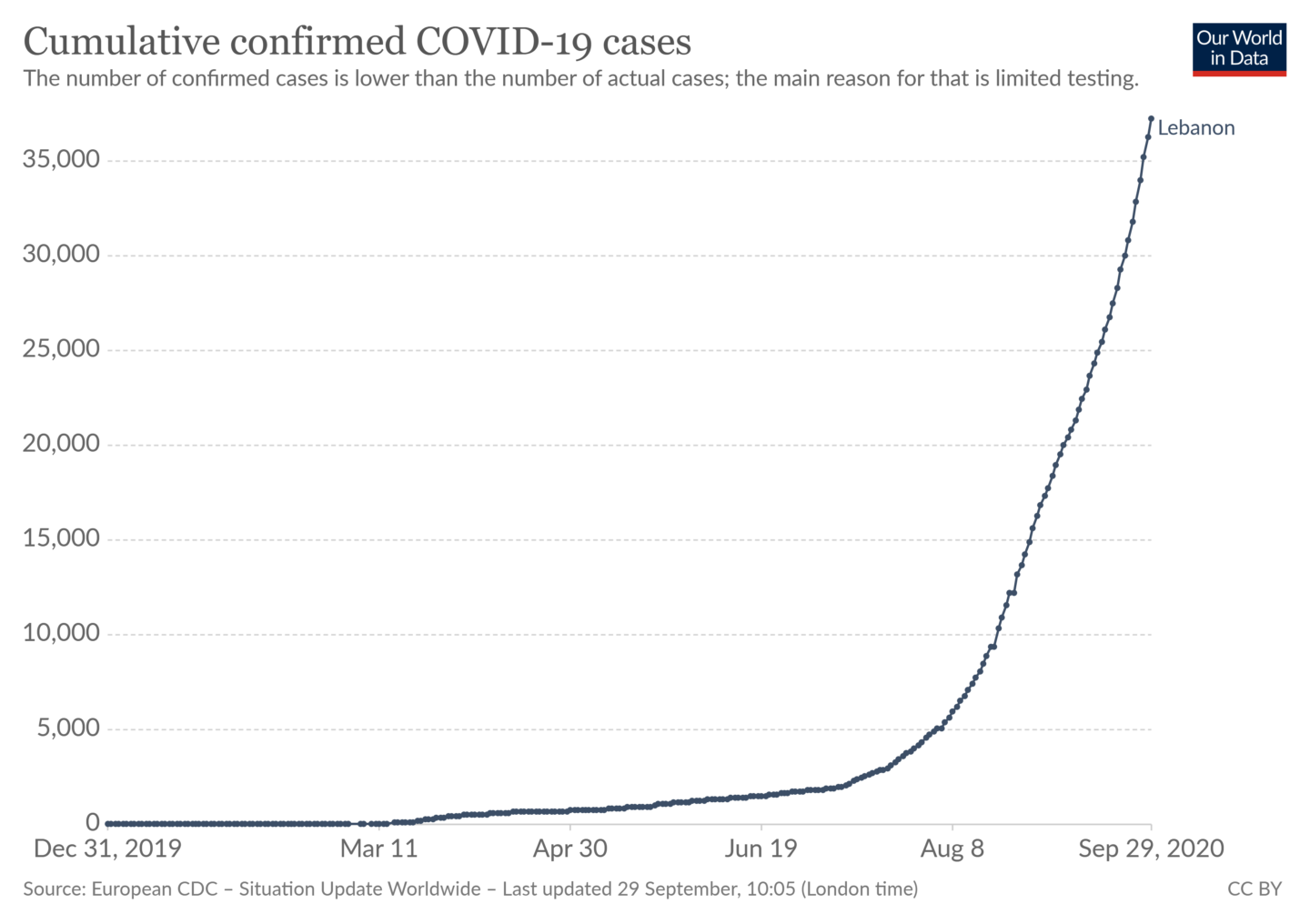
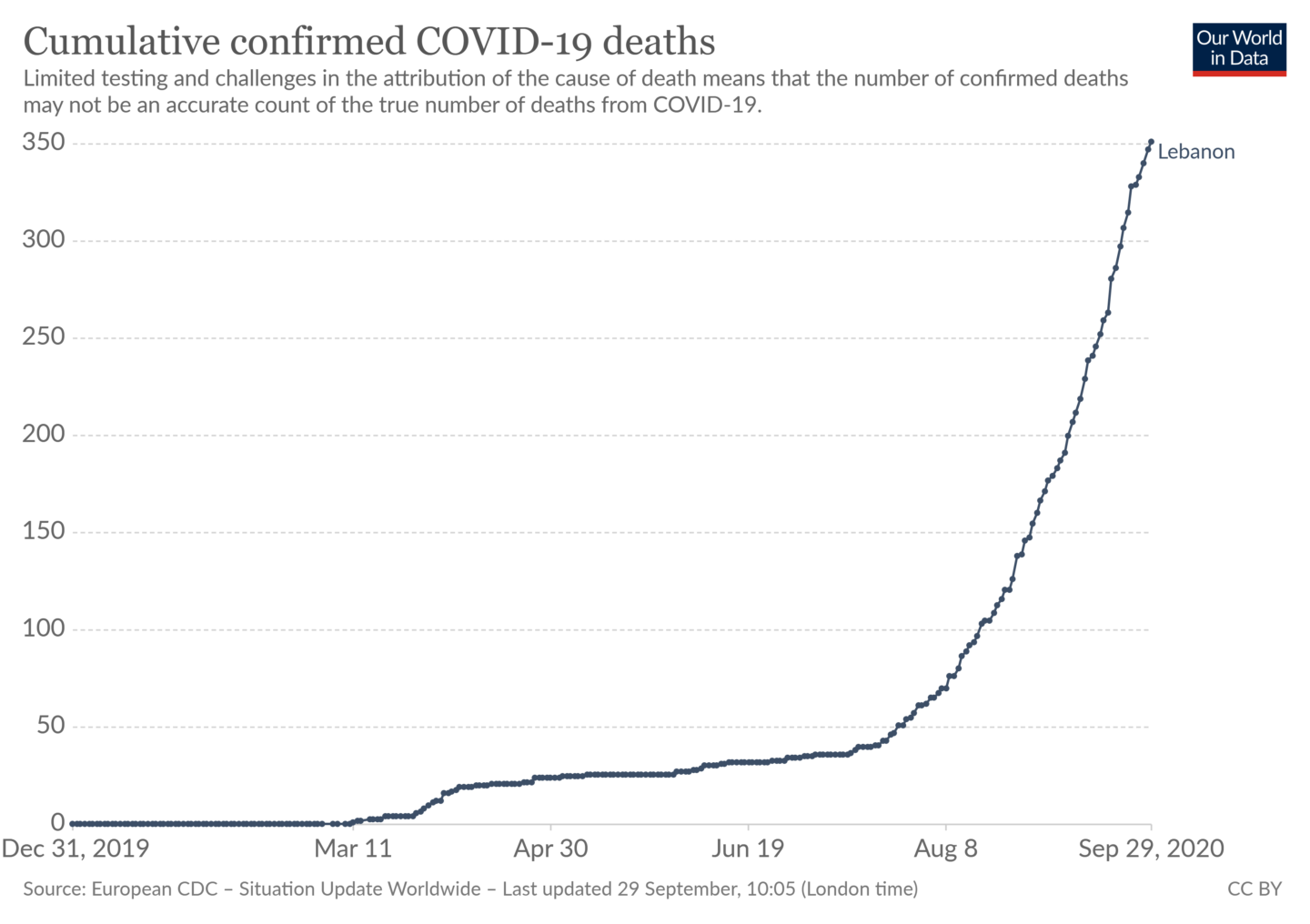
However, the government failed to carry through long-term measures necessary for the maintenance of this early success. It did not adopt policies to assist both an impoverished population and small businesses in facing an unprecedented socioeconomic crisis, which ultimately led to local resistance to strict lockdown measures. Above all, the government failed to develop a long-term strategy to counter the pandemic despite repeated calls and widespread knowledge that the novel coronavirus was going to remain a threat beyond 2020. The majority of cases and deaths have occurred in the past 4 weeks (see figures below), in the absence of clear interventions and consistent communication with the public. We, the Independent Lebanese Committee for the Elimination of COVID-19 (zerocovidlb.com), a group of concerned citizens with various health-related expertise, have come together to sound the alarm and offer paths out of the current crisis. Overall, and in the light of the evolution of COVID-19 in the country, we are highly concerned with the absence of both a clear and comprehensive national strategy and a sound action plan to respond to the critical situation.
In this first report, we address weaknesses in current government policy formulation and then highlight several directions and actions for a more coherent and sustainable national strategy. A series of more pointed policy briefs on some of the issues that are raised here will be published in the coming period.
Current Policy Shortcomings
There is no updated comprehensive national strategy. The government’s approach has been to simply mitigate the impact of COVID-19 rather than eliminate the virus. It succeeded in this respect at the start of the crisis but is now clearly failing. Several countries have adopted the so-called “zero-COVID” strategy, which aims to eliminate domestic transmission. Though this may sound ambitious, it entails decisive and effective intervention for a few weeks, while providing the greatest near-normality for the longer term. We argue that a zero-COVID strategy is even more appropriate for a country of the size and socioeconomic situation of Lebanon and especially given the long-term burden of COVID-19 for many of the survivors.
There is a lack of transparency regarding data. The Ministry of Public Health (MOPH) has a duty to share data with the public. Without such transparency, any trust from the public or scientific community will be limited. It is not enough to publish daily statistical reports, especially when these are incomplete, sometimes even contradictory, and lack information that would be actionable at local levels. The MOPH only shares the number of people infected on incoming flights and the geographical distribution of those infected locally. However, more information is required, such as the context in which people get infected (workplace, home, market, public transportation, refugee camp, prison or unknown), the kind of comorbidities they have, and their socioeconomic status. It would also be helpful to know if people who are taking appropriate precautions are having less severe forms of COVID-19 or not.
More perplexing is the lack of consistent data regarding the numbers of hospitals (public and private), COVID-equipped intensive care units, COVID-dedicated isolation beds, ventilators, and vital stocks in personal protective equipment (PPE), testing kits, medications, antibiotics, antivirals, etc. There are conflicting numbers including those published by the MOPH. In sum, we do not know the available health-system capacity of the country, as well as the underlying factors that are influencing the spread of the virus.
In addition, while the MOPH has a surveillance system in place, the variables, indicators, and epidemiological thresholds it has chosen to monitor and evaluate the spread of the virus are not made public. We believe that making these indicators public would help people recognize even more the importance of social and physical distancing, thereby contributing to reducing the circulation of the virus based on evidence and real-time estimates.
There are numerous unknowns regarding the process of contact tracing. Contact tracing (which includes identifying “cases” and “contacts” that might be infected, providing support, advising on isolation and quarantine, and following up on the evolution/resolution of symptoms) is key to controlling the transmission of the virus and ultimately eliminate it. Although the MOPH has established a hotline for people with COVID-19 symptoms, we have very little information about its overall contact tracing strategy and capacity, as well as the difficulties it has been facing. We do not know how many clusters of outbreaks there are and their evolution since the first case was discovered in February.
There are questions about the validity of testing in different regions. Even though the central laboratory of Rafik Hariri University Hospital is conducting gold standard tests, we do not know whether there are validity measurements of kits being used in other laboratories. The testing conditions do not seem to be respected in peripheral regions, false positive and false negative testing results were repeatedly reported in the media. A random surveillance of testing validity is needed, and its results should be published for the sake of greater transparency and better management.
Towards a Better COVID-19 Strategy for Lebanon
In addition to addressing the weaknesses described above, a more comprehensive strategy would need to take into account the following:
Stronger public communication strategy
It is crucial that the government invests more in informing the public about the necessary steps to reduce the transmission of the virus. Such steps include frequently reminding the public (via televised public health announcements and other means of public-health outreach communications) of the crucial importance of wearing masks, of keeping physical distances, and of reducing social visits and gatherings, be it in the public or private realms (birthday parties, religious gatherings, funerals, weddings, and so on). The importance of televised, online and print media in actively engaging the public in these efforts is crucial in order to maintain trust in public health recommendations and enhance solidarity. While the MOPH has resorted to such means, they are inconsistent and insufficient. There is a lot of misinformation, conspiracy theories, and general lack of trust in the government’s health communications. Some of this “infodemic” is due to ignorance and to the comfort that conspiracy theories can bring in times of uncertainty, while other sceptical attitudes are due to more legitimate reasons that have to do with the opacity of data and lack of transparency.
Better coordination and collaboration with local authorities
Given the difficulty of implementing any lockdown due to the dire economic situation, measures should be taken in consultation with municipalities and local authorities to counter the surge in cases and cut the transmission of the virus from Beirut to the various cities and villages. This is crucial as internal movement within the country is highly prevalent given that Lebanon is a very small country. High traffic – high-density areas such as Beirut are more likely to be susceptible to virus transmission than rural areas and villages. This leads us to consider the concept of “green-zoning,” a strategic approach that has been used in several countries to separate zones that have the virus under control from those that do not, ultimately allowing greater freedom of movement and economic activities.
We find the recent news of the government’s intention to apply some aspects of green-zoning encouraging, which is in part due to the advocacy of our members throughout the past week. Any geographical information allows greater response at local levels. However, we note our concern regarding the acute lack of information regarding this initiative, its use of ratios instead of the number of absolute cases, whether it would limit movement from red towards other zones, and the lack of coordination with municipalities. We also emphasize the need for appropriate communication of official information, away from over-reliance on social media or newspaper paywalls.
A more comprehensive strategy for education and awareness
School re-openings have been postponed once again with no comprehensive strategy. We hope that this is to give the caretaker government enough time to frame a plan regarding the education of an increasingly impoverished population that cannot afford online education. At the same time, the country cannot afford to lose a generation due to the pandemic. “Blended education” is admirable but will be hard to achieve in the absence of economic assistance or relief packages to families in need and given the frequent shortage of electricity and internet connection instability.
Reinforced border control
Although measures were put in place in the spring to control the borders (land, sea, air) and mitigate this route of propagation, this no longer seems to be the case. It is certain that the low effectiveness of quarantine and isolation among airport arrivals has contributed to seeding the virus throughout the population. The extent of this is unknown, given the limited data provided. Nevertheless, it is notable that an increasing trend of cases began shortly after the Beirut airport returned to high-level operations on July 1, 2020. There have been several cases of non-compliance with post-arrival home quarantine and isolation requirements, with false negatives likely contributing to the spread. This is exacerbated by local customs of mass visits of arrivals by family members and friends.
A wider social safety net
The government has put together a meagre economic package (amounting to less than 1% GDP) to try to offset the impact of the shock of the COVID-19 crisis. The epidemic crisis and the ongoing economic crisis have pushed half the population into poverty. The recent Beirut explosion further deteriorated the situation. In addition, Beirut lost half its tertiary hospital capacity, diminishing the already precarious hospital capacity of the country. The Ministry of Social Affairs is running a very small social safety net, covering for now about 50,000 very poor families. This is far from meeting the number of households in need, which is estimated to be 356,000 according to the World Bank, including poor and extremely poor households (amounting to about 2 million people). Since the Beirut explosion, the government has not updated this economic program, nor has it shared any additional plan on how it seeks to offset the additional burden caused by the blast. Lockdowns and other restrictions will not be respected in the absence of adequate social safety nets.
In light of the above, and our recognition that a national elimination strategy is indispensable in defeating the threat of COVID-19 and in saving countless of lives, the Independent Lebanese Committee for the Elimination of COVID-19 extends its arms to everyone willing to help eliminate COVID-19 in Lebanon. Let us join together our efforts and act.
Joelle M. Abi-Rached, MSc, MD, PhD
Nahla Issa, PhD
Jade Khalife, MD, MPH, MSc
Pascale Salameh, MPH, PharmD, PhD, HDR
Ayah Karra-Aly, BA, MMASc
Michèle Kosremelli Asmar, MHA, PhD
The views represented in this paper are those of the author(s) and do not necessarily reflect the views of the Arab Reform Initiative, its staff, or its board.