While the World Health Organization (WHO) supports a policy of widespread testing for COVID-19, different countries are pursuing very different testing strategies depending on the availability of tests, the state of the pandemic in the country, and the capacity of local health authorities to administer the tests.
This paper focuses on Lebanon’s testing approach. It argues that given the limited testing resources, fragmented and under-financed healthcare system (especially in the public sector), and dire economic circumstances which make a long-term confinement strategy difficult to sustain, Lebanon’s approach should focus on testing vulnerable groups (e.g., over 60 years old; people with chronic conditions) and those who are at higher risk of getting infected and spreading the disease (e.g., healthcare professionals, food service and transportation workers). Such a testing policy would need to be accompanied by a targeted quarantine for infected individuals.
Lebanon’s current testing approach
The first case of COVID-19 in Lebanon was confirmed on 21 February. At the time, the government assigned Rafik Hariri University Hospital (RHUH), a public hospital in Beirut, as the main (and at the time, only) site that would test for COVID-19 and admit infected individuals. Until mid-March, testing was limited to RHUH labs, and the tests were offered at no charge. A large cluster of cases was then identified in the north following one case in the Matn region, and as such, a testing site was opened at one of the regional private hospitals. By the beginning of April, the government has expanded testing capacity and added more sites reaching a total of 16 sites by 8 April.
By increasing sites, Lebanon managed to increase its daily capacity of testing from a maximum of 250 tests/day (until 31 March) to 500 tests/day as of 1 April. As of 14 April, Lebanon has conducted a total of 14,007 tests.
Although testing is currently available at 16 hospitals, these are primarily concentrated in urban areas, with very limited or no access to testing in almost all rural areas in Lebanon (Figure 1). Tests are free at RHUH, and cost ranges from 150,000LBP – 200,000LBP (approx. $100USD depending on applicable exchange rate) at the other 15 sites. Additionally, only symptomatic and suspected cases are currently being tested.
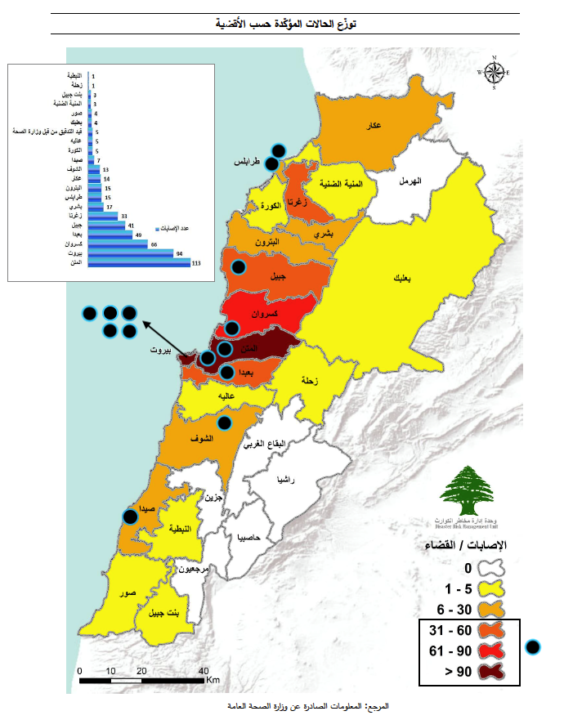
Figure 1: Distribution of testing sites in Lebanon (Source: Ministry of Public Health - only Arabic available)
In principle, the testing approach applies to Lebanese and non-nationals, including Syrian and Palestinian refugees. Health Minister Hamad Hassan said that the responsibility for refugee health care should be shared between the Lebanese government and UN agencies. UNHCR, the UN refugees agency, said that it would cover the costs of testing and treatment for COVID-19 for Syrian refugees in any treatment centre, but only after the health ministry’s screening and recommendation. UNHCR also indicated that it would fund additional wards with additional beds, including additional intensive care units so there is sufficient response capacity for all communities, Lebanese and refugees alike. As of 5 April, just one Palestinian and three Syrians, all of whom live outside the camps, had tested positive for COVID-19, out of 520 infections and 17 deaths across Lebanon.
What is the state of the outbreak in Lebanon?
In assessing Lebanon’s testing strategy, it is essential to understand the stage of the outbreak the country is in. Massive testing for people with symptoms can play a decisive role in containing the virus in the early stages. This was the case of South Korea which succeeded in containing the outbreak early on by implementing a large and well-organized testing programme combined with extensive efforts to isolate infected people and trace and quarantine their contacts.
Lebanon, like most other countries, missed this early window of opportunity, which led to an increase in the proportion of community transmission. Despite support from the WHO and some European countries in terms of testing kits, it is unlikely Lebanon will have the capacity to increase testing sufficiently enough to help identify and isolate as many cases as possible and then adopt control measures to fully tame the outbreak.
But all is not lost, and Lebanon’s containment and other measures seem to have been successful in delaying the surge of the outbreak. As of 14 April, there are 641 confirmed COVID-19 cases and 21 related deaths in Lebanon. These numbers suggest that the virus is spreading but that its growth rate (which can be approximated by examining the doubling time, i.e., the time it takes for confirmed cases to double) is slower than it would be without taking any measures, and is suggestive of a flattening epidemic curve.
The validity of these conclusions depends on the quality of reported numbers, which are likely an underestimation. The actual number of cases can never be determined exactly because the authorities cannot test the entire population. Many infected individuals could be asymptomatic and, in the case of Lebanon, testing sites are not available in rural areas and their cost may deter many people from coming forward. One possible way to try to estimate the potential number of cases is to use the case fatality ratio (CFR), which represents the proportion of deaths compared to the total number of confirmed cases for a certain period. CFR varies on a daily basis and as the number of cases and deaths changes; the only stable CFR can be calculated when the outbreak ends. When this approach is applied to the number of deaths in Lebanon, results suggest that current reported numbers are an underestimate of the actual number of infected people by a factor of 3 to 5. These results raise an important question; if there are so many under-reported cases in Lebanon, why are we not seeing a surge in hospitalizations? A possible explanation to this lies in the fact that the vast majority of cases in Lebanon are in younger age groups, who often have a mild case that does not require hospitalization. This under-reporting of – likely mild or asymptomatic – cases may not have an impact in the short term in terms of health system capacity; however, it will have important implications in the long-term with respect to lifting the lock-down without understanding the actual scope of spread within the community. If there is a large number of undetected cases, these individuals can continue to infect others, ultimately reaching vulnerable groups when the lock-down is lifted. Testing to identify as many cases as possible is crucial in understanding the extent of community spread to plan a safe lifting of the lock-down and gradual return to normal life.
So, Lebanon finds itself like many other countries adopting a mixed strategy of containing as much as possible while trying to mitigate the impact of the virus. The question then becomes, what role should testing play in such a strategy? The answer depends on the resources and capacities of Lebanon.
Between the ideal and the possible: Some difficult choices for Lebanon
COVID-19 is both a health and an economic crisis, and the whole world is in a situation where trade-offs between the lives of some people and livelihoods of others are being made. This is exceptionally challenging given Lebanon’s recent economic turmoil. A lock-down is unsustainable over months without various socio-economic support measures. Despite the plans and promises by government officials, nothing in terms of an economic support package has materialized so far.
Ideally, Lebanon would ramp up testing dramatically while expanding its geographic coverage, notably in rural areas, to try to get a better handle on the spread of the virus in the country. The increase in testing would be accompanied by a more wholistic approach to trace contacts of those identified as infected by COVID-19 and quarantine them. This would then allow for the rest of the economy to gradually open.
This approach of increased testing for the entire population would be appealing if Lebanon’s health infrastructure can follow and the state can monitor all identified cases. Some back of the envelope calculations would suggest that Lebanon would not be able to implement such a policy. Even if it found a way to dramatically increase testing, its health infrastructure would quickly be overrun.
What if Lebanon is unable to ramp up its testing capacity to the level required?
An alternative approach for Lebanon would be to focus its limited testing capacity towards vulnerable groups (e.g., over 60 years old; people with chronic conditions), and those who are at higher risk of getting infected and spreading the disease (e.g., healthcare professionals, food service and transportation workers). In parallel, testing should be expanded into rural areas, where the quality of healthcare services remains poor and access to them, limited in order to enable the identification of any cases among vulnerable populations. Even with centralized testing sites, options like mobile or drive-through testing where samples are collected and transferred into a centralized lab for processing are feasible in a small country like Lebanon. Also, the current clinician-administered process of obtaining a sample significantly limits testing capacity and puts frontline healthcare workers at risk of COVID-19 exposure, particularly that personal protective equipment will need to be changed every time a sample is obtained from a suspected case. For that, some have proposed self-swab testing as an approach to enhance testing capacity and protect healthcare workers. This could be done along with targeted quarantine of high-risk groups and opening up the economy to low-risk groups for a period of time until herd immunity is achieved.
Such an approach, of course, requires exceptional coordination of efforts within all levels and across various divisions of the government, as well as utmost transparency that could enhance public’s trust and cooperation with government efforts. The question remains, can Lebanon meet these requirements?
The views represented in this paper are those of the author(s) and do not necessarily reflect the views of the Arab Reform Initiative, its staff, or its board.
